Legg-Calvé-Perthes Disease (LCPD) is a type of osteochondrosis affecting children, primarily between the ages of 2 and 12, with a higher incidence in those aged 5 to 6 and a greater prevalence in boys. This condition involves the degeneration and subsequent regeneration of the epiphysis, or growth end, of a bone. Specifically, LCPD impacts the head of the femur, the upper portion of the thigh bone, which fits into the hip joint. The disease is characterized by a temporary loss of blood supply (ischemia) to the femoral head, resulting in avascular necrosis and deformation of this bone segment.
Clinical Description and symptoms
| Classification Level | Disorder |
| Prevalence | 4-5/100,000 |
| Age of Onset | Childhood, mainly boys |
| Inheritance | Multifactorial COL2A1 gene mutations – autosomal dominant |
LCPD manifests through symptoms such as limping, pain in the hip, knee, thigh, or groin, muscle spasms, and restricted hip movement. Although the cause of the temporary blood flow interruption is not entirely understood, most cases appear to occur sporadically without a clear reason. The disease process is often self-limiting, as new blood vessels form (revascularization) and healthy bone tissue gradually replaces the damaged area (re-ossification).
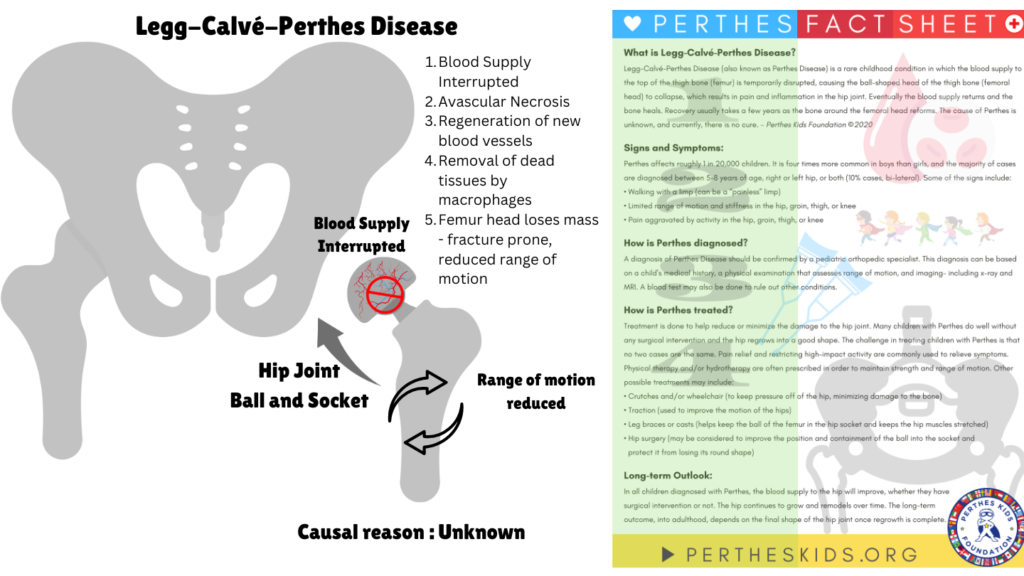
Image I: Overview of Legg-Calve-Perthes Disease
Diagnosis and Current Treatment
LCPD diagnosis typically involves conventional X-rays, with additional use of scintigraphy, ultrasound, and MRI when necessary. Differential diagnoses include Meyers dysplasia, multiple epiphyseal dysplasia, and spondyloepiphyseal dysplasia according to Orphanet.
The goal of treatment of LCPD is to keep the femoral head properly positioned within the acetabulum, either through abduction braces or surgical procedures. Recent research indicates that femoral osteotomy may offer better outcomes than braces like the Scottish Rite abduction orthosis. Prognosis varies, with factors such as the extent of femoral head necrosis and residual deformity influencing the long-term outcome. Severe deformation can increase the risk of early-onset osteoarthritis, and some cases may require total hip replacement in early adulthood. Generally, a younger age at diagnosis is associated with a more favorable outcome.
Treatments can range from supportive or nonoperative Treatment which focuses on a) maintaining hip joint movement is crucial as it provides synovial fluid, which nourishes the cartilage on the femoral head b) keeping the femoral head properly positioned in the hip socket helps it reshape correctly as new bone forms. Treatment may involve casting, bracing, or physical therapy to assist in maintaining this position. Surgery is generally not recommended for children under 6 years old. For older children, the goal is to contain the femoral head within the acetabulum to promote normal spherical growth. An osteotomy may be performed, involving adjustment of the femur and/or acetabulum to correct the bone’s alignment.
Traditional treatments have limitations in effectively promoting bone regeneration. BMP2, a growth factor known to stimulate bone formation, has been proposed as a potential therapeutic agent. A recent study published in Regenerative Medicine by Harry Kim, M.D., M.S. et al used Bone morphogenetic protein-2 (BMP2) incorporated into a hydrogel matrix to locally deliver the growth factor and improve bone regeneration. This method provides an effective localized delivery system for BMP2, leading to enhanced therapeutic outcomes compared to traditional treatment options. The findings suggest potential for this approach in clinical settings and warrant further investigation to optimize treatment protocols and evaluate long-term benefits.
For more on therapeutics against this disease, stay tuned for L for Legg-Calvé-Perthes Disease part II. Meanwhile, click here for more available resources and support groups for Legg-Calvé-Perthes Disease.
Dr. Malini Gupta, Ph.D.
Sources
- https://www.nature.com/articles/s41536-023-00322-2
- https://rarediseases.org/rare-diseases/legg-calve-perthes-disease/
- https://www.orpha.net/
- Image inspired from – https://www.youtube.com/watch?v=zSs16h_k58g
- Image contains fact sheet from – https://www.pertheskids.org/
Disclaimer
The editors take care to share authentic information. In case of any discrepancies please write to newsletter@medness.org
The sponsors do not have any influence on the nature or kind of the news/analysis reported in MedNess. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of MedNess. Examples of analysis performed within this article are only examples. They should not be utilized in real-world analytic products as they are based only on very limited and dated open-source information. Assumptions made within the analysis are not reflective of the position of anyone volunteering or working for MedNess. This blog is strictly for news and information. It does not provide medical advice, diagnosis or treatment nor investment suggestions. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
MedNess is a part of STEMPeers® which is a 501(c)(3) organization registered in PA as PhD Career Support Group. The organization helps create a growing network of STEM scientists that is involved in peer-to-peer mentoring and support.

