Although a rare muscle disorder, Duchenne Muscular Dystrophy (DMD) is one of the frequent genetic disorders affecting male births globally. More than 30 different muscle dystrophies are known, of which DMD is classified as Dystrophinopathy, a progressive muscle degeneration disease caused by the deficiency of Dystrophin. DMD is caused due to mutations in DMD gene which encodes the muscle-specific isoform Dp427m, producing defective dystrophin leading to the severe symptoms associated with the disease. Due to its very large size, with 79 exons, the DMD gene is prone to random spontaneous mutations. A crucial protein that acts as a cushion during muscle contractions, in its absence, muscles progressively weaken and sustain damage, losing their ability to self-repair after injury.
Dystrophin resides in the sarcolemma of skeletal muscle serving as a crucial link between cytoskeletal F-actin with extracellular matrix and is part of the dystrophin-associated glycoprotein complex. The exact mechanism through which dystrophin deficiency initiates muscle fiber degeneration remains unclear, but in its functional or physical absence, sarcolemma gets destabilized leading to wilting of the membrane. This eventually leads to the leakage of creatine kinase into the extracellular matrix and the import of Calcium ions leading to eventual cell death. As time passes, affected children encounter challenges with walking and breathing, ultimately facing failure of the heart and respiratory muscles.
Orphanet Description and Clinical Features
| Classification Level | Disorder |
| Worldwide Prevalence | 1-9/100, 000 |
| Age of Onset | Childhood |
| Inheritance | X-linked recessive |
- Onset typically begins in early childhood, with affected boys often experiencing delayed walking (after 18 months of age) along with speech and/or global developmental delays.
- Commonly observed are autism spectrum disorder and behavioral issues like ADHD, anxiety, and obsessive-compulsive disorder.
- Without treatment, boys with DMD seldom achieve the ability to run or jump, and the condition progresses rapidly which include a waddling gait, positive Gowers’ sign, difficulty climbing stairs, and frequent falls.
- Loss of independent ambulation typically occurs between 6 and 13 years old, with an average age of 9.5 years in non-steroid-treated patients.
- Untreated patients usually succumb to respiratory failure or cardiomyopathy during their late teens to early twenties.
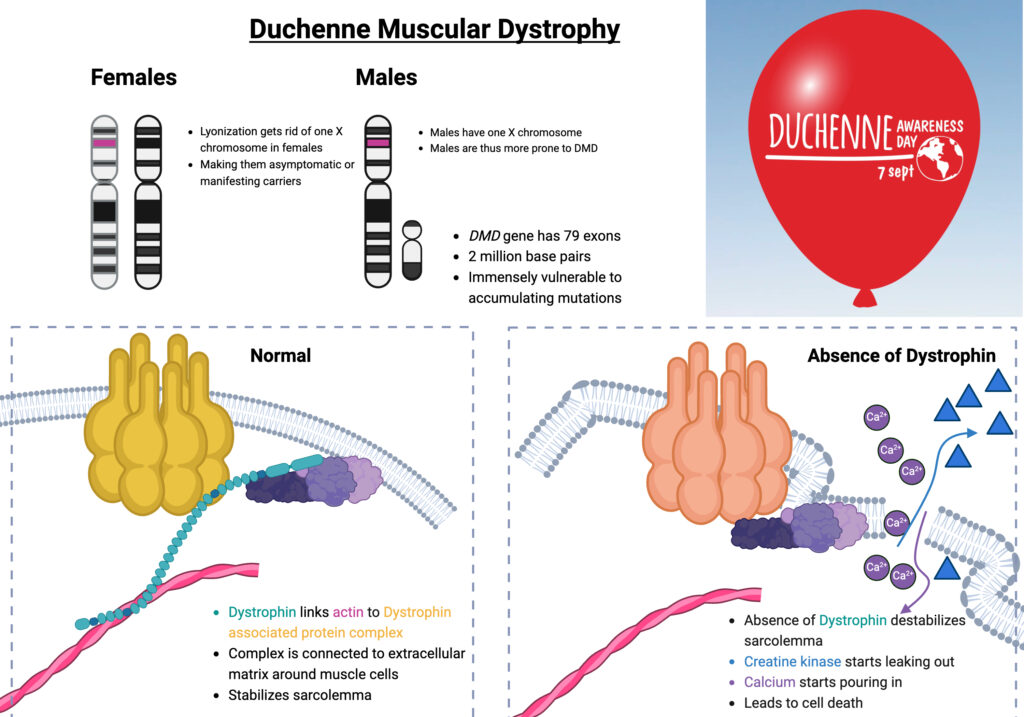
Figure 1: Duchenne Muscular Dystrophy; Image Source: Malini Gupta
Diagnosis and Current Treatment
DMD has a harsh prognosis and life expectancy is significantly reduced with death in the third to fifth decade. Diagnosis is based on clinical presentation, family history, and laboratory findings like 100-200X elevated serum creatine kinase levels. The gold standard for diagnosis is genetic testing, utilizing multiplex-ligation-dependent probe amplification (MLPA) to detect exon deletions and duplications and gene sequencing to identify mutations. Muscle biopsy is recommended if genetic analysis is inconclusive, offering additional diagnostic insight. Differential diagnoses usually involve Becker muscular dystrophy and limb-girdle muscular dystrophy.
Management for conditions like Duchenne muscular dystrophy involves:
- Physiotherapy: Passive stretching and nighttime AFO for tendo-Achilles contractures.
- Corticosteroid Therapy: Prednisolone, prednisone, or deflazacort from age 4-5.
- Ophthalmic checks for cataracts/glaucoma
- Cardiac Care: Regular monitoring (echo/MRI), ACE inhibitor/beta-blocker treatment
- Respiratory Management: Monitor respiratory function, BiPAP for sleep hypoventilation.
Dr. Malini Gupta, Ph.D.
Sources: